Case presentation
A 47-year-old right-handed man presented with weakness of the left side of face, arm and leg. He had had a few glasses of alcohol in the evening, then he had a nap on the sofa for two hours and when he woke up his family noticed that he was confused and unable to move his limbs. He had no past medical history nor has he a family history of stroke. He has never smoked but he used to drink a few glasses of alcohol on the weekends. His Glasgow Coma Scale (GCS) was 14/15 (E4, V4, M6) and he had dysarthria, left facial drop, left upper extremity weakness (1/5), left lower extremity weakness (2/5) and sensory loss on the left side of the body. His National Institutes of Health Stroke Scale (NIHSS) was scored as 12 and his computed tomography (CT) head was normal. In view of these clinical and radiological findings and the fact that 3.5 hours had elapsed since the last time he had been normal, the patient was thrombolysed with alteplase.
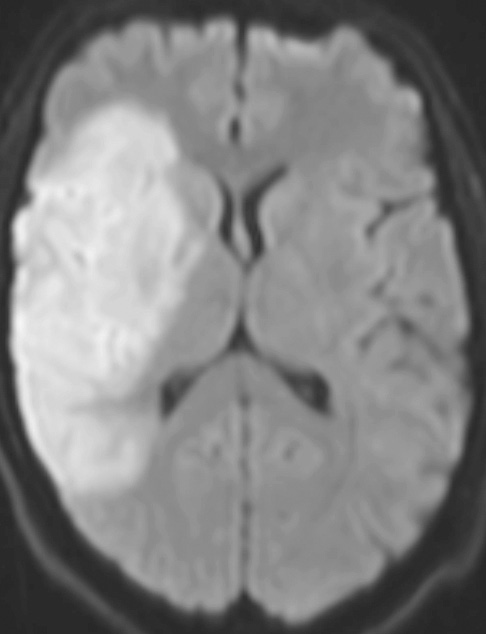
Next morning, a magnetic resonance imaging (MRI) scan of the head confirmed a large right middle cerebral artery territory infarction secondary to thrombus (Figure 1).
Figure 1 MRI diffusion-weighted imaging (DWI) showing a large area of restricted diffusion in keeping with a right middle cerebral artery territory infarction
His investigations for stroke in a young patient were all normal including HBA1c, lipid profile, folic acid, vitamin B12, thyroid function test, autoimmune profile, echocardiography and seven days electrocardiogram (ECG). To rule out dissection, the patient had a computed tomography angiography (CTA) from arch to vertex which interestingly showed bilateral elongated styloid processes with the tip of the right styloid process contacting the cervical right internal carotid artery (ICA) and causing a focal narrowing of the artery (Figure 2).
Figure 2 CT angiography showing bilateral elongated styloid processes which measures nearly 4cm in length on the right side. The tip of the right styloid process contacts the cervical right ICA and causes a focal narrowing of the artery
Four days into admission, his GCS dropped to 11/15 (E3, V3, M5). His repeated CT head revealed expansion of the oedema of the right MCA infarction with mass effect over the adjacent parenchyma and lateral ventricles. In respect to this, the patient had decompressive hemicraniectomy and was discharged two months later with a modified Rankin score of four at discharge.
Discussion
An elongated styloid process of more than 3cm affects about 4% of the population but most of them are asymptomatic.1 In symptomatic patients, the clinical manifestations associated with elongated styloid process characterise Eagle’s syndrome, first described by Dr Watt Eagle in 1937.2
The classic Eagle’s syndrome is characterised by orofacial and neck pain without vascular involvement, while stylocarotid syndrome depicts compression of the external carotid or internal carotid arteries by elongated or deviated styloid process.3 This encroachment on the carotid arteries can result in dissection formation, occlusive or stenotic carotid lesions, pressure-induced plaque formation or plaque rupture.4
Three-dimensional CT angiography (3D-CTA) is considered the imaging modality of choice for diagnosis of stylocarotid syndrome due to its ability to detect the elongated styloid process and its compressive effect on the adjacent blood vessels.4 Interestingly, dynamic CTA by adopting certain neck positions as neck flexion can be invaluable in some circumstances when it is difficult to demonstrate a relationship between the elongated styloid process and the surrounding blood vessels in neutral neck position.1 In addition, colour Doppler flow imaging and transcranial Doppler that can be done with provocative manoeuvres are useful in detecting the haemodynamic changes within the affected arteries. Hence, it can be helpful in confirmation of the diagnosis as well as assessment of successful treatment.5
There is no consensus on the best method of treatment of stylocarotid syndrome. While the styloidectomy seems to be a reasonable choice to prevent recurrent strokes, conservative management by educating the patient to avoid the positions that may provoke impingement on the carotid arteries is another option.6
Conclusion
Clinicians should keep in mind stylocarotid syndrome as a cause of stroke which could range from minor strokes to severe disabling strokes. CTA is the diagnostic imaging modality of choice and provocative manoeuvres by gentle neck rotation can be considered to establish the diagnosis in difficult cases. 
Acknowledgements
The author would like to thank Dr. Adnan Fazal (stroke consultant) for his useful suggestions.
References
1 Brassart N, Deforche M, Goutte A et al. A rare vascular complication of Eagle syndrome highlight by CTA with neck flexion. Radiol Case Rep 2020; 15: 1408-12.
2 Eagle WW. Elongated styloid processes: report of two cases. Arch Otolaryngol 1937; 25: 584-7.
3 David J, Lieb M, Rahimi SA. Stylocarotid artery syndrome. J Vasc Surg 2014; 60: 1661-3.
4 Eraslan C, Ozer MA, Govsa F et al. Relationship of stylohyoid chain and cervical internal carotid artery detected by 3D angiography. Surg Radiol Anat 2017; 39: 897-904.
5 Esiobu PC, Yoo MJ, Kirkham EM et al. The role of vascular laboratory in the management of Eagle syndrome. J Vasc Surg Cases Innov Tech 2018; 4: 41-44.
6 Shindo T, Ito M, Matsumoto J et al. A case of juvenile stroke due to carotid artery dissection from an elongated styloid process - revisiting conservative management. J Stroke Cerebrovasc Dis 2019; 28: 104307.