Introduction
Traditionally, students enrolled in medical programs such as MBBS and BDS are taught anatomy courses that include cadaveric dissection, which enables students to examine the organs in the human body systemically and topographically. Although textbooks, models, charts, and computer programs are all excellent supportive factors, cadaveric dissection assumes a unique role in assisting students to understand the complexities of the human structure and function. First exposure to cadaveric dissection is often a significant emotional event in the lives of young medical students accompanied by a variety of mixed feelings.1 There are varying responses as regards their attitudes and views towards cadaveric dissection, some literature suggests that students encounter trauma symptoms and that female students might be more prone to exhibiting these symptoms than males,2 while others found that medical students are enthusiastic and find it an effective tool for learning.3
Acute stress disorder (ASD) can be defined as having the same symptoms as post-traumatic stress disorder (PTSD) except that the symptoms last for 1–3 days, whereas PTSD symptoms may last for much longer and might be more severe or get worse over time. Symptoms for ASD prominently include recurrent distressing thoughts and dreams related to the traumatic incident, contact psychological stress, avoidance of reminders, disturbed sleep, restlessness, cognitive difficulties such as with concentration and memory, and a persistent negative mood.4 Symptoms of ASD are valuable to study because they can often advance into PTSD; patients with ASD symptoms are at a risk of developing PTSD in the next 6 months.4
There has not been much research conducted in the area of cadaver dissection in south Asia. However, research from Taiwan, Nepal, and other Asian counties suggests that cadaver dissection causes physiological and psychological symptoms in students. For example, Tseng and Lin5 conducted research in a medical school in Taiwan and found that students adopted a defense mechanism called ‘detachment’, students detached all emotions from the cadaver and treated it like an object instead of a human, which hindered learning. Similarly, Khan and Mirza2 recorded that most of their sample experienced physical symptoms and were distressed during the first dissection. Out of this sample 11% (about 19 students) had to see a doctor for these symptoms. Fear and nausea were the most common types of symptoms found during dissection in Ethiopia.6
However, most research suggests that anxiety or anxiety symptoms often improve in students over time after the first dissection. Agnihotri and Sagoo1 estimated that though dissection caused anxiety in their sample, the symptoms improved within 6 weeks. Wisenden et al.7 found that students in the West experienced anxiety upon first-time dissection, but the symptoms faded over time. However, non-white, non-Christian students continued to face anxiety during dissection throughout the semester. To counter this, the researchers offered them humanization training, and though this improved their anxiety, it made anxiety in the females worse. Qamar et al.8 concluded females remain more stressed throughout medical school. Overall males report feeling more prepared compared with females, but significant gender differences are not usually found in the levels of anxiety faced by medical students in first-time dissections.3
Arráez-Aybar et al.9 carried out a study in a teaching hospital in Madrid, Spain. They measured anxiety pre- and post-dissection in first-year students via the State Anxiety Scale of State Trait Anxiety (STAI) and the Situation and Responses Anxiety Inventory (ISRA). Anxiety levels were significantly different before and after dissection, they peaked before and during dissection but decreased after the students had left the dissection hall. A repetition in anxiety measurement after the students had been exposed to a second-time dissection showed that anxiety had greatly reduced before, during, and after compared with the first time. A significant finding from their study was that students who had perceived the situation as threatening were most likely to have high scores for anxiety on the STAI and ISRA. Similarly, Curfman et al.10 found that in a sample of physical therapy students in Virginia, PTSD symptoms were present for the first dissection but reduced with continuous exposure to dissections.
Quince et al.11 conducted a study on 156 medical students. They found that students with high scores for depression and anxiety, those recently bereaved, and those who tested higher for death anxiety showed a negative attitude towards dissection.
Interestingly, despite experiencing psychological and physical symptoms, most students believed that cadaver dissection was an important learning tool. From the study mentioned above, Quince et al.11 reported that 60–94% of their sample had positive attitudes towards dissection. In Khan and Mirza’s2 sample, 80% of respondents said that they believed cadaver dissection was a better learning tool than plastic models. Despite the symptoms recorded in Mulu et al.’s study,6 99% of the sample agreed that dissection was very important for learning.
This study measured the psychological impact of cadaver dissection by assessing the presence of ASD in the sample via scores on the Impact of Event Scale-Revised. The Appraisal of Life Events Scale was used to measure the perceptions participants had about their first cadaver dissection. This included whether the participants perceived the situation to be threatening or stressful, or whether they had positive perceptions about it. The Death Anxiety Inventory was used to measure if the event of dissection induced death anxiety among the participants.
This study had four objectives:
- To explore if first-time exposure to cadaveric dissection can lead to first-year medical students developing acute PTSD symptoms known as ASD. To see how students who had developed these symptoms had perceived the dissection at the time. In other words, what sort of perception was necessary to invoke traumatic symptoms.
- If death anxiety was also present in students with ASD.
- If there were gender differences in the occurrence of ASD symptoms. Some of the research discussed in the introduction and literature review has hinted that female students might be more likely to develop symptoms of stress and anxiety during medical school.2,8
- This study aims to see if female students are also likely to display symptoms of ASD post-cadaveric dissection.
Methods
The study was conducted in Lahore, Pakistan. Using a random sampling technique, a sample of 135 medical students from two prominent teaching hospitals in Lahore was selected. The sample size was calculated using the expected percentage of any psychological problem as 93.06% and keeping a 5% margin of error and 95% confidence level or level of significance (p < 0.05). Data were analysed by employing a simple linear regression and Pearson’s correlation, in addition to descriptive statistics. All statistical analyses were run on IBM-SPSS version 23. The authors have quoted the numerical findings in the results section and used the existing literature to interpret these findings qualitatively. Qualitative explanations for the results have been elaborated in the discussion section.
Participants were first-year students who had recently experienced their first cadaver dissection. Students who had a history of psychological illness, psychiatric medication, or had already had exposure to cadaver dissection before were not included. Mean age of respondents was 19.1 years [standard deviation (SD) = 1.13], 73 (54.1%) were male and 62 (45.9%) were female. Respondents were provided with an information sheet explaining the objectives of the study, followed by an overview of their right to withdraw and information about confidentiality and protection of their personal information. All participants were asked to sign their consent and then fill out a questionnaire consisting of the following three scales, keeping their first cadaver dissection in mind.
The Impact of Event Scale-Revised (IES-R) is a questionnaire used to determine the amount of trauma a person experiences after a specific situation. Generally, a score above 33 is considered to be enough to make a diagnosis for PTSD.12,13 This was used to measure if PTSD symptoms were present in our sample.
The Death Anxiety Inventory (DAI) measures how afraid one is of death or situations related to dying or dead bodies. Scores range from 15–75, where low death anxiety is 15–35, moderate death anxiety is 36–55 and high death anxiety is 56–75.14 This was used to measure death anxiety to see if it had any correlation with ASD symptoms.
The Appraisal of Life Events Scale-Revised (ALE-R) has three subcategories. ‘Threat’ measures how harmful or anxious the situation was perceived to be. ‘Challenge’ measures how much potential a situation was perceived to have for growth and mastery. ‘Loss’ measures how depressing or negative a situation was perceived to be.15 This was used to measure how the respondents perceived the cadaver dissection.
Ethical approval
Ethical approval for the study was obtained from The Board of Studies in Medicine, King Edward Medical University on 19 August 2017 via order no 748-750/EMW/KEMU/17.
Results
Results were scored and measured using IBM-SPSS version 23. A simple linear regression was used to see what percentage of the DAI and the ALE-R subscales predicted the scores on the IES-R. Therefore, scores on the IES-R were held constant as the dependent variable, and scores for DAI and ALE were held as independent variables. Simple linear regression was employed to see to what extent scores on the independent variables predict the scores on the independent variable.
The mean score for the IES-R was 36.15 (SD = 15.99), three points above the cut-off score needed to diagnose PTSD (33). Linear regression analysis showed that the Threat domain (β = 0.509, p < 0.001) and the Loss domain (β = 0.216, p = 0.005) on the ALE-R scale were the largest predictors of a high IES-R score (Figure 1), meaning that students who scored high for these two were more likely to have symptoms of ASD. Challenge (β = 0.193, p = 0.012) on the ALE-R scale, was the smallest predictor meaning that it had little to no impact on determining if students developed ASD symptoms, and the DAI made no prediction (β = 0.021, p = 0.769) (Figure 1). The overall model fit was R2 = 0.440. Table 1 summarises the regression results.
Figure 1 Percentage of each variable score on Impact of Event Scale-Revised (EIS). ALE, Appraisal of Life Events Scale; DAI: Death Anxiety Inventory
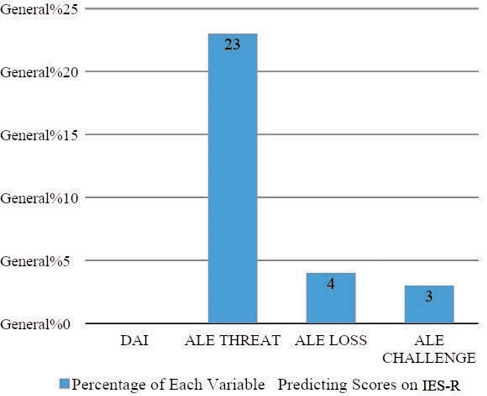
Table 1 Regression results
|
|
|
|
|
|
|
|
Constant
|
20.739
|
15.531–25.946
|
|
7.896
|
0.000
|
|
DAI
|
0.004
|
-0.022–0.029
|
0.021
|
0.294
|
0.769
|
|
ALE-Threat
|
0.992
|
0.698–1.286
|
0.509
|
6.693
|
0.000
|
|
ALE-Loss
|
0.029
|
0.009–0.048
|
0.216
|
2.901
|
0.005
|
|
ALE-Challenge
|
0.408
|
0.012–0.093
|
0.193
|
2.564
|
0.012
|
Females who scored higher on the IES-R also scored higher on the DAI (R2 = 0.347, p = 0.014) but no significant correlation was found between DAI scores and IES-R Scores. IES-R positively correlated with Threat on the ALE-R (R2 = 0.595, p < 0.001). This was true for both genders. There was no significant correlation established with Challenge and Loss on the ALE-R scale. The adjusted R2 value showed that overall, ALE-R and DAI were responsible for 41.9% of the variance on the IES-R.
Discussion
This study confirms the presence of ASD symptoms in students following first-time cadaver dissection. Most studies had found that first-time cadaver dissection elicited stressful emotions,2,3 for example, Mulu et al.6 concluded that 75% of their sample of medical students agreed that cadaver dissection was very stressful.
The results show that students who perceived the cadaver dissection as threatening, harmful or anxious also tested high for ASD symptoms. Students who perceived the situation as depressing and negative also scored high on the ASD but not as high as those who perceived it to be threatening. This is in line with the findings from Arráez-Aybar et al.9
Death anxiety itself played no role in predicting higher scores for ASD symptoms, but females who scored higher for death anxiety also seemed to have higher scores on the IES-R. This was the only significant correlation found between the variables. This is also in line with previous literature that suggests that females usually exhibit more symptoms than males during and after cadaver dissection.2,8
Quince et al.11 also found that higher scores for death anxiety were correlated with higher scores for PTSD symptoms, but our study has only found this to be true for females. However, Quince et al.’s study11 also took into account recent bereavement. Their sample filled out the Anxiety and Depression Scale and the Death Anxiety Scale. Students with high scores for depression and anxiety, students who had been recently bereaved and students who tested higher for death anxiety showed a more negative attitude towards dissection.
Research has established that medical students in Pakistan are subject to immense stress. For example, Rehmani et al.16 found that students at Aga Khan University scored higher than the cutoff score for both the student-life stress inventory and the Aga Khan University anxiety and depression scale. Some students also reported suffering from mild depression. Similarly, female students from the University of Medical Dental College in Faisalabad reported high levels of stress due to frequent examinations, poor quality food in mess halls and sleeplessness, among other factors.17 Perhaps the high levels of expectations and stress imposed on medical students in Pakistan lead to an increased susceptibility to negative after effects of cadaveric dissection. Future studies can aim for a more robust analysis by controlling for other stressors (such as academic stress and stress arising from sleeplessness, poor nutrition and living away from home) to isolate the impact of cadaveric dissection on students.
A limitation in our study was excluding students who had been going through psychiatric treatments or had a history of psychiatric illness. Future research should aim to study the impact of cadaver dissection in such students because they may experience more lasting symptoms than typical students.7 It would also be valuable to repeat the scale administrations on the students throughout their first year to see if and how ASD symptoms change over time; do they remain the same or reduce, as suggested by several studies.2,6,11
In conclusion, ASD symptoms were present in first-year Pakistani medical students after their first-time dissecting a human cadaver; symptoms were more prevalent in females. This supports literature collected from south Asian and Hispanic communities. The presence of ASD symptoms in students may lead to hindrance in learning. Exposure via media, photographs, videos, among others, before dissection can reduce the onset of these symptoms9 and should be used to sensitise students to the dissection process. 
References
1 Agnihotri G, Sagoo MG. Reactions of first year Indian medical students to the dissection hall experience. NJIRM 2010; 1: 4 –9.
2 Khan HM, Mirza TM. Physical and psychological effects of cadaveric dissection on undergraduate medical students. JPMA 2013; 63: 831–4.
3 Leboulanger N. First cadaver dissection: stress, preparation, and emotional experience. Eur Ann Otorhinolaryngol Head Neck Dis 2011; 128: 175–83.
4 American Psychiatric Association. Desk reference to the diagnostic criteria from DSM-5. APP; 2014.
5 Tseng WT, Lin YP. “Detached concern” of medical students in a cadaver dissection course: a phenomenological study. ASE 2016; 9: 265–71.
6 Mulu A, Muche A, Tegabu D. Assessment of the attitude and views of second year medical students towards cadaver dissection in anatomy course. Ethiop J Health Biomed Sci 2010; 2: 111–7.
7 Wisenden PA, Budke KJ, Klemetson CJ et al. Emotional response of undergraduates to cadaver dissection. Clin Anatomy 2018;31: 224–30.
8 Qamar K, Kiani MR, Ayyub A et al. Higher stress scores for female medical students measured by the Kessler Psychological Distress Scale (K10) in Pakistan. JEEHP 2014; 11.
9 Arráez-Aybar LA, Casado-Morales MI, Castaño-Collado G. Anxiety and dissection of the human cadaver: an unsolvable relationship? Anatomical Record Part B 2004; 279: 16–23.
10 Curfman SE, Austin GP, Nicholas JS. Post-traumatic stress and academic performance among entry-level doctoral physical therapy students in a human anatomy cadaver dissection course. IJAHSP 2018; 16: 1.
11 Quince TA, Barclay SI, Spear M et al. Student attitudes toward cadaveric dissection at a UK medical school. ASE 2011; 4: 200–7.
12 Weiss DS. The impact of event scale: revised. In: Cross-cultural assessment of psychological trauma and PTSD. Boston: Springer; 2007. pp. 219–38.
13 Hyer K, Brown LM. The impact of event scale–revised: a quick measure of a patient’s response to trauma. AJN 2008; 108: 60–8.
14 Tomás-Sábado J, Gómez-Benito J, Limonero JT. The death anxiety inventory: a revision. Psychological Rep 2005; 97: 793–6.
15 Ferguson E, Matthews G, Cox T. The appraisal of life events (ALE) scale: reliability and validity. BJHP 1999; 4: 97–116.
16 Rehmani N, Khan QA, Fatima SS. Stress, anxiety and depression in students of a private medical school in Karachi, Pakistan. PJMS 2018; 34: 696.
17 Tariq S, Jawed S. Perceived stress, severity and sources of stress among female medical students in a private medical college in Pakistan. JPMA 2020; 70: 162–7.