A previously well 35-year-old vegetarian female presented with generalised progressive increase in bulk of muscles with a bodybuilder-like appearance over six months with no complaint of weakness, fatigue or pain. On examination, the muscles were firm, non-tender and symmetrically hypertrophied in both upper and lower limbs along with weakness particularly in proximal muscles. She also had multiple soft, non-tender nodules of variable sizes on the forehead and neck (Figure 1).
Figure 1 Herculean appearance due to increased bulk of muscles of neck, back and upper and lower limbs (A and B). Nodular subcutaneous swelling in neck (C) provided a clinical clue towards deposition disease.

List of probable differentials included androgen-producing tumours, hypothyroidism, inflammatory myositis, muscular dystrophy, myotonia congenita and infiltrating diseases like cysticercosis.1 All blood workup (including creatinine phosphokinase, relevant hormonal and autoimmune profiles) was normal, except for eosinophilia (total leukocyte count 8,100 with differential eosinophil count 9.6%) and raised C-reactive protein (34.9 mg/L; n<6). Magnetic resonance imaging of limb muscles followed by whole body screening showed the presence of generalised deposits of cysticercus larvae (Figure 2). Excision biopsy of the right calf muscle was performed, with histopathology revealing cysticercus larvae in the muscles (Figure 3).
Figure 2 Magnetic resonance imaging showing multiple well-defined ring-enhancing lesions which are hyperintense in T2-weighted sequence (A, B and G) with perilesional oedema in T2 FLAIR (C) and hypointense in T1-weighted sequence (D, E and F) in all limb muscles, abdominal and paravertebral muscles, neck, tongue, facial and extraocular muscles, bilateral cerebrum and cerebellum suggestive of inflammatory granuloma, most likely disseminated cysticercosis. There is also generalised hypertrophy of muscles.
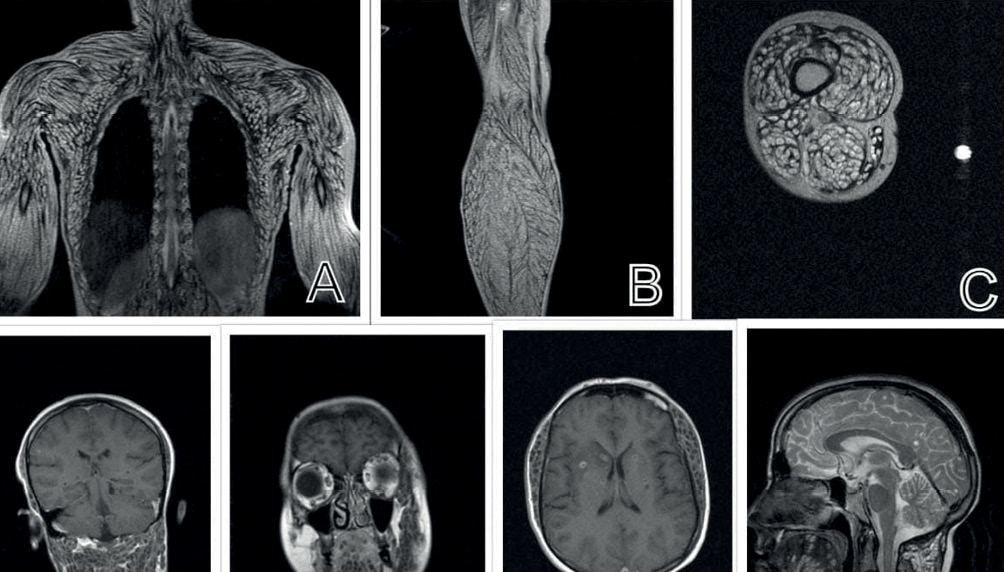
Figure 3 Haematoxylin and eosin staining of the muscle biopsy specimen (taken from right calf muscle) showing cysticercus larvae.
She was treated with albendazole 400 mg tablets once a day under the coverage of dexamethasone 8 mg once a day for two weeks. After two weeks, the dexamethasone was tapered off while the albendazole was continued. Antiepileptic (levetiracetam 500 mg) was added.
Cysticercosis should be considered as the differential of muscle hypertrophy in tropics.2 While disseminated cysticercosis often presents with focal central neurological manifestations (such as headache, seizures, impaired cognition and paresis), symmetrical muscle hypertrophy as the only clinical manifestations is extremely rare.3 The larvae act as irritants, causing inflammatory changes and leading to painless, diffuse and symmetrical muscle hypertrophy.2,3 In this case, subcutaneous nodules found in the neck provided a clinical clue for early diagnosis.